
This insights post is a summary of the blog post published by Madchatter. View the full article at: The Permission Problem: Why Healthcare and Pharma PR Is Won Before the First Pitch Is Sent.
There is a quiet assumption in our profession that healthcare and pharma communications are ordinary PR with a compliance layer bolted on top: write the press release, clear it through medico-legal, soften the claims, and proceed as usual. That assumption is the single most expensive mistake an agency can make in this sector. Healthcare PR is not regulated marketing. It is the management of credibility under conditions where the audience is structurally predisposed to distrust you.
Consider the terrain. India is now the third-largest producer of pharmaceuticals by volume, supplies roughly one in five generic medicines sold worldwide, and exported about $30.5 billion USD in drugs in 2024-25 to more than 200 markets, including the most heavily regulated regimes on earth. The domestic market alone is projected to climb from around $50 billion USD today toward $130 billion USD by 2030. Yet the very scale that makes the sector commercially formidable also makes its communications uniquely fragile: the more lives a product touches, the less tolerance there is for a narrative that turns out to be wrong.
This piece is not an introduction to healthcare PR. It assumes you already know how to run a media list, draft a backgrounder, and respect an embargo. It is about the things that separate practitioners who survive a decade in this niche from those who quietly rotate out: the permission problem, the translation problem, the proxy problem, and the silence problem. Each is illustrated with work our team has handled directly.
1. The Permission Problem: Credibility Is a Prerequisite, Not an Outcome
In consumer or technology PR, awareness usually precedes trust. You make people aware of a thing, and trust accrues later through experience. Healthcare inverts this. A clinician, a regulator, or a health journalist begins the conversation from a position of methodical scepticism, not because they are hostile, but because their professional duty is to assume a claim is unproven until the evidence is overwhelming. The communicator’s first job is therefore not to be heard. It is to earn the standing to be heard at all.
What this changes in practice: the work shifts upstream, long before any outreach. The team that wins in healthcare PR is the team that has done the reading that understands the mechanism of action, the trial design, the regulatory pathway, and the unmet clinical need well enough to anticipate the first three questions a sceptical expert will ask. If your spokesperson cannot survive those three questions, no amount of message discipline will save the story.
“The communicator’s first job is not to be heard. It is to earn the standing to be heard at all.”
This is why the most useful internal metric in early-stage healthcare PR is not reach or share of voice. It is a question of survivability: how deep into expert scrutiny a narrative can go before it breaks. Generalist teams optimise for the headline. Specialist teams pressure-test the footnote, because in this sector, the footnote is where credibility lives or dies.
2. The Translation Problem: Carrying Science Across an Audience Gap Without Distorting It
The defining technical skill in deep-science healthcare PR is translation under constraint: rendering a genuinely complex advance into language a mainstream audience can absorb, without sacrificing a single point of scientific accuracy. Lose the accuracy, and you lose the experts. Keep the jargon, and you lose everyone else. The narrow path between those failures is where the craft sits.
Case in point: positioning a stem-cell therapy innovator
Our work with Eyestem, a company advancing stem-cell therapy, is a clean example of the problem in its hardest form. The communications challenge was not a shortage of news; it was a cluster of compounding difficulties that generalist PR playbooks simply do not account for:
- The science was hard to carry. Stem-cell therapy advances do not compress neatly into a 600-word announcement. Oversimplify, and you misrepresent the science; explain it fully, and you lose the desk editor.
- The timelines were long. Clinical development runs in years, not news cycles. The newsroom rewards events; the science offers slow, conditional progress. Manufacturing a milestone where none exists is how agencies destroy a client’s credibility in this space.
- The regulatory environment was unforgiving. Healthcare communications carry real constraints on what may be claimed about safety and efficacy. Every sentence has a compliance shadow.
- The innovation read as “too niche.” Biotech breakthroughs are routinely dismissed by mainstream desks as specialist concerns with no broad readership.
The resolution did not come from better media relations. It came from a better understanding. The team invested the time to learn the underlying technology, the science behind the treatment approach, and the broader healthcare problem the company was actually trying to solve. That depth unlocked the move that mattered: reframing the story away from “a scientific breakthrough” a frame that interests only specialists, toward narratives a general audience and a health editor both care about:
- Unmet patient need the human problem the science addresses.
- Affordability and accessibility whether the advance reaches people who currently have no option.
- India’s rising capability in advanced healthcare innovation a story of national consequence, not a lab note.
“The breakthrough is the reason the scientist cares. The patient, the cost, and the country are the reasons everyone else does.”
The transferable principle: in deep-science healthcare PR, the breakthrough is rarely the story. It is the credential that earns you the right to tell the story the audience is built to care about. The agency’s value is not in announcing the science; anyone can do that badly. It is in locating the human, economic, and national stakes that the science sits inside, and doing so without overstating what the science can yet deliver.
3. The Proxy Problem: Building Authority When Journalists Want to Talk to Someone Else
A structural reality of pharma media relations is rarely stated plainly: journalists usually want to speak to manufacturers and operators, not to advisors. When a reporter is writing about the sector, the perceived primary source is the company that makes the drug, runs the plant, or manages the supply chain. Anyone positioned one step removed from a consultancy, an advisory firm, or a services partner has to overcome a default assumption that they are not where the real insight lives. This is the proxy problem, and it is one of the hardest positioning challenges in the sector.
Case in point: building thought leadership for a consulting firm in pharma
Establishing Vector Consulting Group, India’s largest homegrown management consulting firm, with pharma clients including Lupin, Glenmark, Ajanta Pharma, Intas and Strides, as a credible thought leader in the pharma space ran directly into this wall. Commenting on the industry at a broad level would only have confirmed the journalist’s suspicion that the firm was a commentator rather than a source. The approach had to change at the root.
Instead of speaking about the industry, the programme spoke from inside it. Vector’s own primary research became the engine: a distribution study spanning over 900 chemists and 68 stockists across 18 cities. The findings were specific enough that no manufacturer could dismiss them as outside commentary:
- Even leading pharma companies achieved only 60–85% brand reach at chemists.
- One in four prescriptions went unfulfilled because the prescribed brand was not on the shelf.
- Companies carried high inventory, roughly 15 weeks in the supply chain and 7 weeks with distributors, yet still saw stockouts.
- The cost showed up as obsolescence and annual inventory write-offs of 4–10%.
Crucially, the insight was attributed to a named operator, not an anonymous “industry view.” As Chandrachur Datta, Partner at Vector Consulting Group, framed it, companies assume that large stock volumes and big stockists guarantee availability, when the reality is the opposite. That single reframe, backed by survey data, is what gave editors a reason to treat the firm as a source.
“India’s pharmaceutical market is growing rapidly, yet the backbone of its distribution remains fragmented.” Chandrachur Datta, Partner, Vector Consulting Group
The narratives were extracted from practice, not opinion, each mapping a board-level concern the manufacturers were already living:
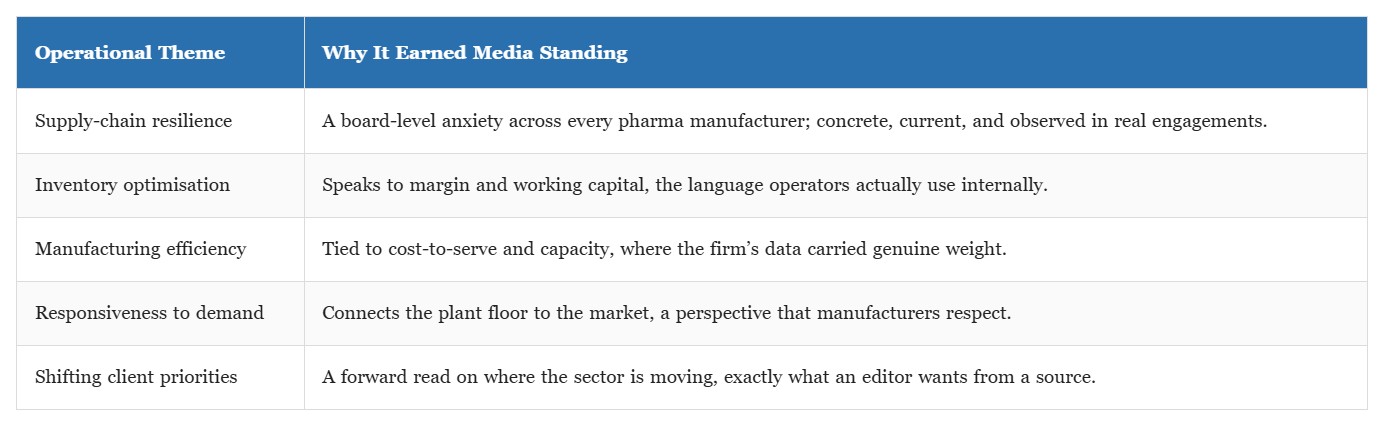
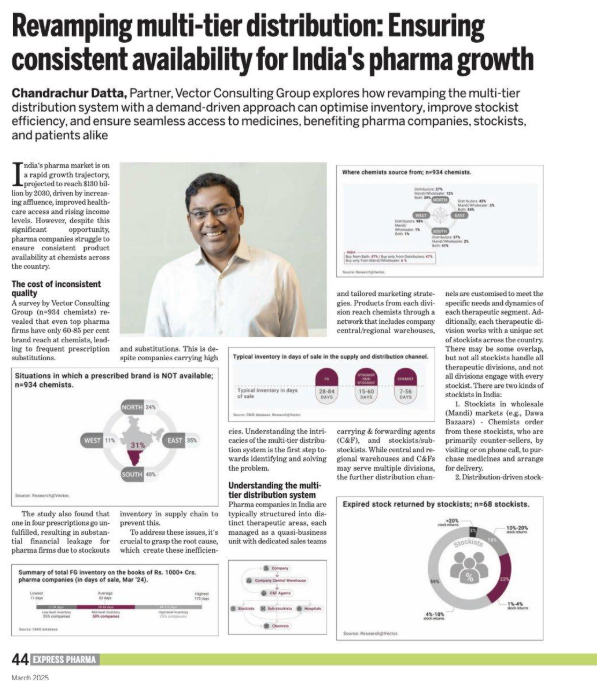
Earned coverage: bylined feature by Vector’s Chandrachur Datta in Express Pharma (March 2025), built on the firm’s own distribution research, the survey data, charts and named partner converting an advisor into a primary source.
The effect was to move the conversation from company-specific intervention to industry-wide insight. The firm was no longer asking to comment on the sector; it was supplying the sector’s own patterns back to it, evidenced by practice. That is what converted a “proxy” into a primary source in the eyes of the press, culminating in bylined, data-led features in trade media such as Express Pharma. A consulting-led perspective rooted in practical experience and data is precisely what makes a non-manufacturer relevant and valuable to a pharma journalist.
“You do not earn standing in pharma by commenting on the industry. You earn it by handing the industry back a pattern it recognises but had not yet named.”
4. The Silence Problem: Designing for the Crisis You Cannot Yet See
The final discipline that separates veterans from newcomers is the willingness to build for failure before there is any failure to manage. In most consumer sectors, a bad week is reputational. In healthcare and pharma, a bad week can involve a recall, a regulatory observation, an adverse-event signal, or a quality finding with consequences for patients, not just perception. The communications function that only activates when something breaks has already lost the most important asset it had: the credibility it built in calmer times.
Three principles that hold up under pressure in this sector:
- Credibility is collateral. Every accurate, restrained, non-overclaimed statement made in good times is deposited against the day a difficult statement must be made. Agencies that inflate ordinary news are spending a reserve they will desperately need later.
- Silence is a message. In a regulated, patient-facing context, a delayed or absent response is read as evasion or incompetence. The discipline is to have pre-aligned holding positions, medico-legal pathways, and spokesperson readiness in place before they are needed so that speed never comes at the cost of accuracy.
- Accuracy outranks speed, always. The instinct to respond fast must be subordinated to the obligation to respond correctly. A fast statement that later proves wrong does more damage than a measured statement issued an hour later.
None of this is glamorous, and none of it shows up in a coverage report. But it is the substructure on which everything visible rests.
5. What an Operator-Grade Healthcare PR Brief Actually Looks Like
Pulling the four problems together, here is how a senior healthcare/pharma PR engagement differs from a standard corporate one. The contrast is where the expertise becomes legible.


Effective public relations in healthcare and pharma is not a louder version of effective PR elsewhere. It is a different discipline, governed by a different physics. The audience starts from doubt. The science resists simplification. The regulators set hard limits. The stakes are measured in patients. And the people you most want as champions, the manufacturers and operators, are the very people journalists would rather hear from than you.
The agencies that endure in this niche are the ones that treat all of this not as friction to be managed but as the actual substance of the work. They do the reading. They reframe the breakthrough into the human stake. They convert the proxy position into a primary source by speaking from evidence. And they build the credibility reserve quietly, so it is there when a hard day arrives. In a sector built on trust, communication is not the wrapper around the product. It is part of the infrastructure of trust itself.
To get more details and insights, read the full post at: The Permission Problem: Why Healthcare and Pharma PR Is Won Before the First Pitch Is Sent.
